

TIPS and TOPICS
Vol 2, No.2
May 2004
In this issue
– SAVVY
– SKILLS
– SOUL
– STUMP THE SHRINK
– Until next time
WELCOME!
Welcome to the May edition of TIPS and TOPICS. Unlike big magazines like TIME where you receive the week’s edition before the date on the cover, this humble effort usually comes late in the month. Finding the “spare time” to get this to you often gets lost in other deadlines. But here it is.
SAVVY
Heavy on my mind this month is treatment planning and documentation.
Why? Because I’m working with a major system to help the team promote person-centered, participatory, collaborative, strength-based treatment planning and services. The trick is how to “walk the talk” on these important goals and reflect this in the documentation. Another trick is how to avoid getting caught up in constructing the perfect forms and wordsmithing so we miss the whole point of our work -i.e. tuning into people and helping them improve their lives. Anyone facing a JCAHO or CARF accreditation survey, or an audit by some regulatory agency will identify with the dilemma of pleasing the surveyor, getting the paperwork right, while actually helping the people we serve.
Tips:
- The treatment contract with the client is what drives the assessment and service planning process.
Accreditation, licensure and other standards all uphold expectations such as this:
” The individual plan contains goals and objectives that incorporate the unique strengths, needs, abilities, and preferences of the person served, as well as identified challenges and problems.” (The Commission on Accreditation of Rehabilitation Facilities, CARF, Behavioral Health Standards Manual, July 2003-June 2004, p.60)
The challenge for clinicians (especially those raised in pathology-oriented traditions and disciplines) is how to resist the impulse to quickly list all the problems that seem so obvious and needing treatment > the psychosis, > the impulse control problems, > the anger, > the substance abuse, > the legal problems. It almost seems that very little input is really needed from the client or patient. Problems, goals and interventions are self-evident – > stabilize the psychosis, > establish medication compliance, > chart progress the patient’s compliance with our treatment plan.
Or
> detox the person, > educate about sobriety, > examine negative consequences of continued use, > identify and cope with relapse triggers, > chart whether the person attends prescribed groups and participates or not.
So what does it mean to actually incorporate “unique strengths, needs, abilities and preferences, challenges and problems”?
We are professionals who are skilled in assessment. By training and experience we know what people need to do to improve their lives. However, if change and treatment outcomes could be effective merely by documenting people’s problems and prescribing therapeutic interventions, then we could send out memos to clients and expect compliance, attendance and progress! Unfortunately, many treatment plans do look like the client was only superficially involved. Goals and interventions seem unrelated to where the client is really at regarding their desire for abstinence, interest in anger management, or even if they have a mental health or substance problem.
What is the treatment contract?
It is the consensus or agreement between client and therapist to work together toward the one most important goal the client wants to achieve.
Ask yourself & ask your client:
* What drives this particular person to be willing to even talk to me?
* What would happen if he/she did not follow through with treatment? Would she go to jail? Be kicked out of her family? Be sent to a foster home? Lose her physical or emotional health? Lose her children? Lose his job? Lose his housing?
*Why is this client or family here now?
Approach the client as a motivated person who wants you to help them with what is most important to them at this point in time. That is the treatment contact – pursuit of that one, most important goal. With the treatment contract clear, this then gives shape, meaning and focus to treatment planning.
This is analagous to the architect’s job: to be crystal clear about what kind of house or landscape you want – your unique needs, preferences, interests, challenges and desires. After articulating your goals, the architect proceeds to collaborate on a plan which will direct the building process. The house plan evolves from the interaction of your wants, needs,and preferences combined with the the architect’s expertise, design talent and work experience.
- The client must see how the problems or priorities in the treatment plan are linked to what she or he wants to achieve (Treatment Contract). If the client doesn’t see the linkage, they are likely to drop out of treatment, either literally or figuratively (just ‘doing time’ in a program).
Person-centered treatment planning is not simply searching for some client quote to demonstrate that they participated. The problem statement documented in the treatment plan, or the priorities listed, must make sense to the client. They must be concrete, specific, user- friendly to help clients identify the obstacles to reaching the goal of their Treatment Contract.
For example:
If the Treatment Contract with the client is to help him or her keep their job, then a problem statement like “Knowledge deficit about addiction” or “Poor insight” does not have immediate buy-in for the client.
Better documentation is:
“Wants to stop drinking but continue marijuana use” or “Feels his job is threatened because his boss mistreats him, not because of his absenteeism”.
This ties into a plan around discovering whether continued marijuana use, or blaming his boss, will increase his chance of keeping his job or decrease it.
For example:
If the Treatment Contract is to help the patient get out of hospital as soon as possible and return to independent living, then problem statements like “Psychiatric” or “Substance Abuse” are too general.
Better documentation is:
“Wants to stay in bed all day” or “Punches people when angry” or “Hallucinating and delusional and cannot say what she wants yet” or “Doesn’t want to stop using ice and weed” are better.
These problem statements or priorities are the kinds of obstacles to the client’s reaching the goal of the treatment contract – i.e. returning to the community and living independently. Can the patient see how demonstrating progress in these areas will reassure the treatment team he’s ready to go out on his own? This is the collaborative, participatory process that “walks the talk.”
SKILLS
Here are some clinical tips related to these points:
Tips:
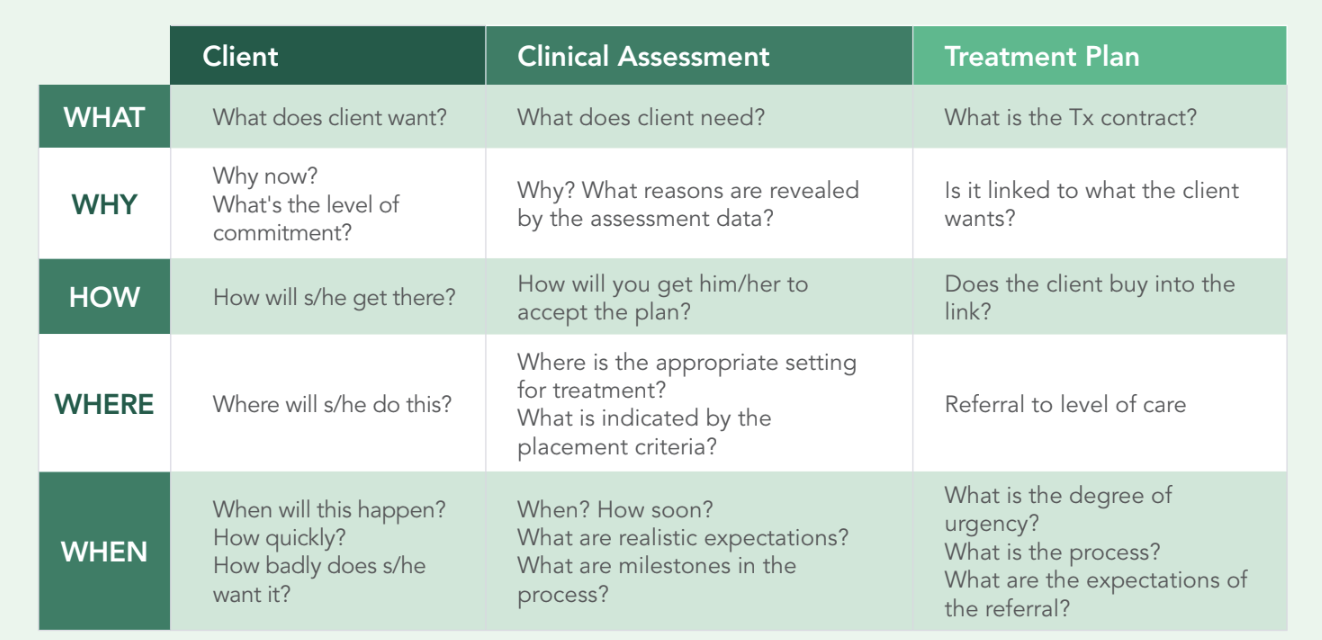
- Explore the “What, Why, How, Where and When” to Develop the Treatment Contract.
We want to develop a truly participatory treatment plan, one most likely to succeed in being followed. First be clear what the client really wants, not what they’ve been told they need; or what you (perhaps correctly) feel they need to change, or what they think the clinician wants to hear. Determining what the client wants means going deeper beneath the surface of a rote presenting complaint like “Depression” or “Brought in by the police”. One method is to ask the “What, Why, How, Where and When”. This explores:
> What a client wants—
> Why the wants are so important to the client & Why now—
> How s/he intends to achieve that goal—
> Where and When s/he is willing to act on the treatment plan.
The police may well have brought in the client, but what the person states is that he wants “to be left alone”. The treatment contract can genuinely be based on this specific “want”.
Client: “I want to be left alone.” Therapist: “I will help you to be left alone.”
Take the client at his/her word. You can then discuss why people are not leaving the client alone, and what he/she would have to do differently to get people to leave him alone.
- Five Key Questions to Develop the Treatment Contract
Q1: What is the agreed upon treatment contract collaboratively arrived at?
Q2: Why now and is the client really committed? Play devil’s advocate. See if you can talk them out of it in case they are just saying what they think you want to hear. Ask: Have I dug deep enough?
Q3. How does the client plan to achieve his/her goal? Do they have their own tenacious treatment plan, which blinds them to your plan? You may have to start with their plan to see if it works.
Q4. Where are they willing to receive treatment? Do they have tenacious ideas about level of care and type of program?
Q5. When are they willing to receive treatment? Do they have tenacious ideas about when to start and the length of treatment?
For more tidbits on Treatment Planning:
Read previous editions of my Tips & Topics.
>> June 03: in Skills section
>> July 04: in Savvy & Skills sections
SOUL
Consider these quotes:
- “I think the relationship that you have —– is critical”
- “The better the relationship ——- the better results are going to be”
- “We can do a lot of things —– but if we don’t have a relationship —–as far as the quality end with them, that will be a real challenge”
- “We go in and say we want to come in and help —– (They) roll up their sleeves and we’ll go in with them and help”
You may think these are quotes on the importance of a participatory relationship with your clients, families, team members or community.
Actually these are quotes from the Chiefs of American Honda Motors, Nissan North America, Hyundai Motor America, and Toyota USA respectively. (USA Today, May 24, 2004 Section B, page 6). They were talking about the importance of the relationship in working with, and improving quality with, their manufacturing suppliers.
We live in a results-oriented world where accountability, audits, regulatory compliance and the big stick seem to rule the day. It is interesting to note that even in the cutthroat competitive auto industry, the consensus is that participatory, collaborative relationships are what bring results and quality.
In treatment planning, documentation, staff teams, family life and who knows -maybe even world affairs- it is participatory, collaborative relationships that are important and effective. As the song says in 1960’s musical “Hair”, it’s “Easy to be Hard”. But it’s not so easy to harness the power of relationship.
STUMP THE SHRINK
Question #1:
” I am struggling with the concept of methadone maintenance treatment coexisting with the 12 step recovery program wherein we promote total abstinence. In your opinion, is someone who is taking methadone in a clinic abstinent? And how can that person be accepted at AA or NA meetings? Having been sober for over 22 years and working in a drug rehab. center for over 6 years as a therapist, I am having a difficult time when people try to tell me methadone should be looked at the same way as a person taking an antidepressant.”
Rehab. Counselor
Answer #1:
I know the issue of methadone maintenance is tricky for many 12 Step abstinence- based programs. Just as there are some people in an abstinence-based who are often just doing time and not working a sober, spiritual growth recovery program, so too are there some people on methadone maintenance who are just doing time on methadone. They may be scared to be off drugs; or are trying to cope with the chaos of being addicted to an illegal drug that requires them to do all kinds of illegal and antisocial things just to survive.
A person with alcohol dependence can be a regular citizen and buy their drug at the grocery store. Methadone can help stabilize a person and stop short the daily antisocial life that a person with an alcohol problem doesn’t have to face since they are addicted to a legal drug.
My point is that someone on methadone in a 12 Step program may not be “abstinent” as they are indeed on a substance, but they could be “in recovery” as they are working to improve their life as regards drug use. We might want them to be perfectly abstinent and sober today, but if they are making progress in recovery, that is still recovery. Recovery is not perfect abstinence – it is an ongoing process that involves physical, mental, social and spiritual growth. I would say that a person on methadone maintenance can do the same growth in recovery that an alcoholic person does in AA or NA and therefore should be welcome in recovery groups like AA.
Of course, as I said, there can be people in 12 Step, abstinence programs who are not in recovery. There can also be people on methadone maintenance who are not in recovery. To me abstinence isn’t the same as recovery and is not the only way to start recovery.
David
Question #2:
“What is the best approach in incorporating the Addiction Severity Index (ASI) with the Patient Placement Criteria?”
Substance Abuse Specialist II
Answer #2:
“The ASI gives you important assessment information that can help you assess the severity and functioning of the client in some of the ASAM six assessment dimensions. So counselors can use the information collected in the ASI to jumpstart the assessment information needed to understand the client’s needs in the ASAM assessment dimensions.
However, the ASI will give perhaps only about 40% of what you will need to understand the client’s multidimensional needs using the ASAM assessment dimensions. For example, if a client has used every day for the past 30 days, that will not tell you for sure if the person has Withdrawal Potential in Dimension 1 of the ASAM Criteria, because the person may have had just one beer a day for 30 days which would not necessarily require detoxification services.
Also, the ASI does not directly explore Readiness to Change (Dimension 4) or Relapse, Continued Use, Continued Problem Potential (Dimension 5). You can infer some of these issues from the ASI, but more assessment questions would be needed to fully assess all the ASAM assessment dimensions. The ASI was never designed to be a comprehensive assessment of all client needs. The ASAM assessment dimensions were developed to try to address all clinical needs of clients.
So, in summary, the ASI and ASAM dimensions can complement each other, but not replace each other for the purposes they were originally designed to achieve. The ASI, as I understand it, was designed to be an outcome tool to assess the success or not of programs to improve functioning in the ASI domains. The ASAM assessment dimensions were designed to assess and treat all relevant biopsychosocial areas of need in addiction (and now with the ASAM PPC-2R 2001 edition) mental health clients.”
David
Until next time
Thanks for reading TIPS and TOPICS.Thanks for the feedback, comments and questions you send.
Until June—
David